

The comfortable alternative
Open and Upright MRI scan
Why choose Vista Health for an Open or Upright MRI scan?
-
Affordable
From only £575. This is a fixed price for one body part.
-
Accessible
Our Open and Upright MRI scans are available in Birmingham and London (Fitzrovia).
-
Fast
With no waiting lists, we can often schedule an appointment for the same day.
-
Maximised comfort
Our Upright Open scanners are designed to provide maximum comfort and a stress-free alternative to an enclosed-tunnel MRI scanner.
-
Claustrophobia
Open MRI can be used to scan most body parts and regions. If you suffer from claustrophobia or another anxiety issue, it could be more comfortable for you than a standard, tunnel MRI.
-
Imaging in Position of Pain
Patients with mobility issues, who are overweight, or who find it difficult to lie down may also benefit from Open MRI techniques. For certain procedures and conditions, it has the advantage of allowing for a variety of positions.
What are the benefits of an Open or Upright MRI scan?

Claustrophobia
Our cutting-edge scanners are specifically built for patients with claustrophobia or other anxiety issues, or who need to be observed during scanning.

Imaging in position of pain
An Upright Open MRI scanner is ideal for scanning various parts of the body in weight-bearing positions. The scanner can be moved to a location that allows for better imaging of the body portion being studied.

Bariatric / restricted mobility
Upright Open MRI scanners are useful for anyone who can't lie flat for long periods of time, or who can't fit comfortably into a typical MRI tunnel scanner.
Optimal image quality, without the ‘tunnel’
An Open MRI scan is an alternative to the conventional MRI and offers optimal image quality for patients who are not comfortable with a conventional scanner.
Our Open and Upright MRI scanners use cutting-edge technology specifically designed for patients with anxiety issues, who are claustrophobic, or who have bariatric or restricted mobility issues.
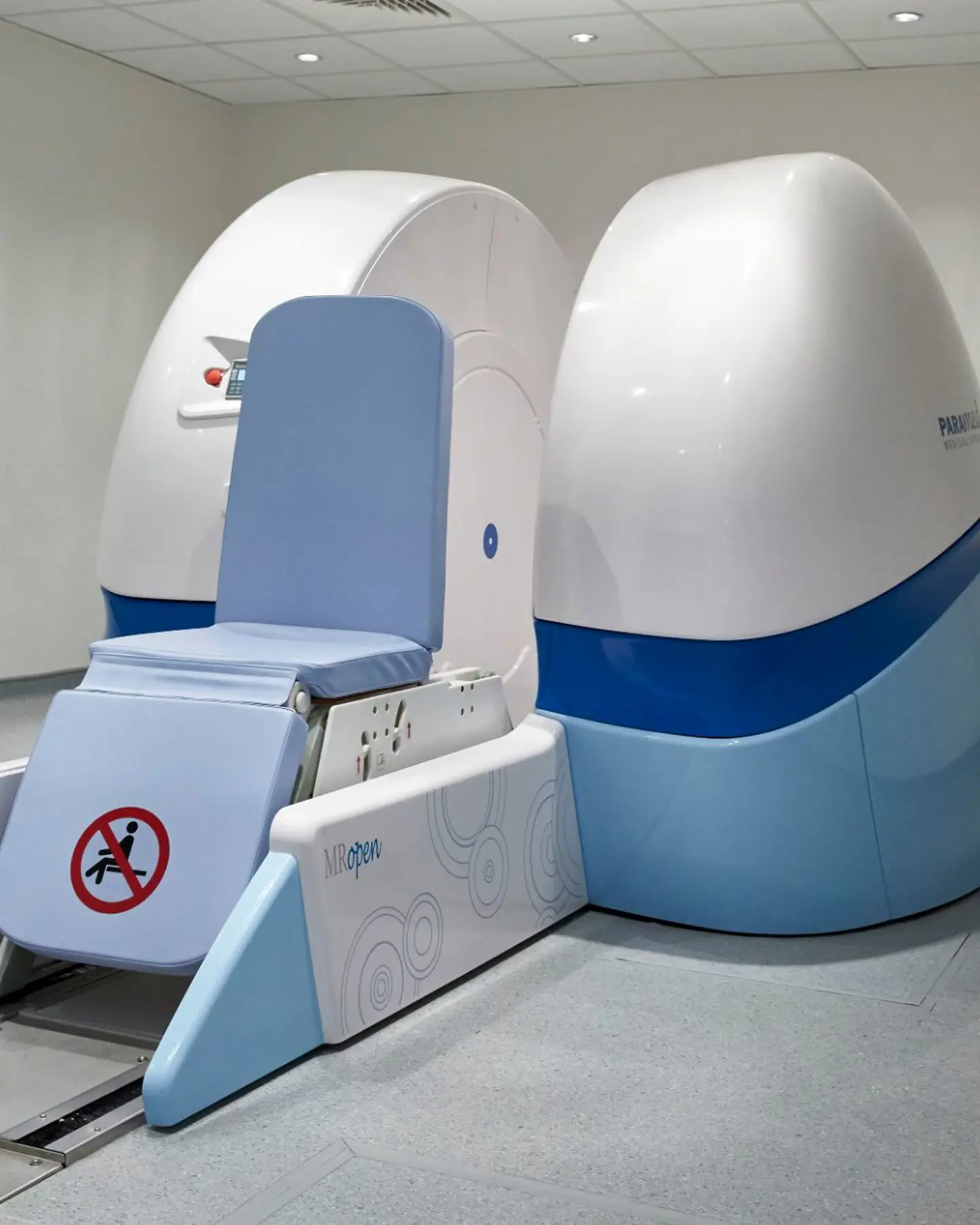
Thanks to the nature of their 'open' design, these machines allow you to sit between two large magnetised plates, and you can look out. It also allows for different scanning positions, such as seated and leaning.


What are Open & Upright MRIs?
Standard MRI scanners are designed like a tunnel or large tube. The patient is enclosed within the tube while the scanner creates images of the body. For some patients - for example those with restricted mobility, who are overweight, or who suffer from claustrophobia - this can be difficult or uncomfortable.
- Open MRI provides a stress-free, relaxing alternative compared to the traditional MRI scanner.
- Open and Upright MRI scans deliver the same level of accuracy as a traditional, ‘tunnel’ scanner.


Advantages of an Open or Upright MRI scanner
Open MRI offers important differences when compared to standard ‘tunnel’ MRI scanning, and can benefit some patients for many procedures.
Open MRI has the advantage of being able to detect issues only visible when the patient is in a weight-bearing situtation, or in a position that causes discomfort.
- Patients can be imaged lying down, standing or sitting. Please note that standing scans are currently available only at our London location and are limited to lumbar spine imaging.
- Ideal for patients who suffer from claustrophobia or anxiety
- Allows patients to be observed during the scan
- Offers a range of different MRI scans including brain, spine, shoulder, ankle, and the pelvic region
- Our Open MRI facility features tranquil landscape pictures on the walls, and a music system which patients can use to enhance overall comfort and relaxation


Specially designed alternatives to standard tunnel scanners

Upright MRI Scan
Our Upright Open MRI Centers utilise state-of-the-art scanners specifically designed for weight-bearing positions. Their 'open' design is particularly beneficial for patients who experience claustrophobia or anxiety.

Open MRI scan
Our newly installed Open MRI is specifically designed for scanning patients in weight-bearing positions. It also accommodates patients lying down, making it an ideal solution for individuals with claustrophobia, anxiety, larger body types, or limited mobility.
How much does private Open or Upright scanning cost?
| Label and description | Value |
|---|---|
|
Birmingham
Upright MRI
|
From £575
|
|
London
Conventional Open and Upright MRI
|
From £600
|
Discover the unique benefits of our Open MRI services
Unlike traditional ‘tunnel’ MRI systems, our newly installed Open MRI is tailored for scanning patients in weight-bearing positions. By allowing patients to be scanned while lying down, it provides an ideal solution for individuals experiencing claustrophobia, anxiety, or those with larger body types or limited mobility.
Our Open MRI technology offers a comprehensive range of scans, including brain, spine, shoulder, ankle, and pelvic region imaging, ensuring quality imaging results.
In addition to its distinct advantages over conventional ‘tunnel’ MRI systems, our facility features tranquil landscapes on the walls, creating a peaceful environment for our patients. We also offer a music system that patients can plug into, enhancing their overall comfort and relaxation during the scanning process.
How can we help?
Support
If you’re about to begin a healthcare journey, you’re likely to have a few questions. We’ve tried to answer the most common queries here - but if you don’t find what you’re looking for, you can always ask one of our friendly patient care advisors.
What is an Open and Upright MRI scan?
An Open MRI scan is an alternative to the conventional ‘tunnel’ MRI and provides optimal image quality. Open and Upright MRI is ideal for certain areas of your body including bones, soft tissue, and brain, and is one of the most innovative imaging methods used to date.
Why may I need an Open and Upright MRI scan?
An Open and Upright MRI scanner is ideal for a variety of patients, including:
- Patients that may suffer from claustrophobia or anxiety
- Patients who need to be imaged in a lying down, standing or in a seated position
- Patients who are larger or have restricted mobility or that are unable to lie down
Where are your Open MRI scanners located?
Our Open and Upright MRI scanners are available in Birmingham and London.
What is the magnetic strength of the Open and Upright MRI scanners?
Our scanners operate the below field strengths:
- Upright MRI (London Fitzrovia) - 0.6T
- Magnifico Open (London Fitzrovia) - 0.4T
- Upright MRI (Birmingham) - 0.5T
Is there a weight limit when having an Open MRI scan?
The weight restrictions for our Open and Upright MRI scans are outlined below:
Leeds/Birmingham Upright MRI:
Maximum Weight: 200kg / 31.5 Stone
Maximum Width: 56cm / 22 inches
London Conventional Open Scanner
Maximum Weight: 200kg / 31.5 Stone
Will I feel claustrophobic during the scan?
An Open MRI unit is ideal for patients with claustrophobia and anxiety. An open MRI machine has an opening far wider than the standard machine, so you can see out both sides.
Our Upright Open MRI is a truly open system that increases relaxation to reduce anxiety. You can walk into the scanner and can even watch television while being scanned.
How long will my private Open or Upright MRI scan take?
The length of your scan session will depend on the body part or region being scanned. As a guide, most Open MRI appointments take about 45 minutes, and we’d ask you to arrive around 15 minutes before your scan.